Our sMRI technology is more advanced than clinically available MRSI
Spectroscopic proton MR imaging (1H-sMRI), which can display the distribution of endogenous metabolites within tumor tissue as a molecular image/map, has been evaluated by various research groups and has shown benefit for the differentiation of neoplasm from non-neoplastic lesions, and for glioma grading. Metabolites that can be reliably evaluated with proton SMRI include, but are not limited to, choline-containing compounds (Cho), which are nearly always elevated in gliomas; creatine (Cr), an energy metabolite; and N-acetyl aspartate (NAA), present in healthy neurons. Early studies established that the spectra obtained from brain tumors differ significantly from those obtained from normal brain, with increased levels of Cho and diminished levels of NAA, suggesting that SMRI can add reliable guidance with high specificity and sensitivity to locate tumor cells. The average Cho/NAA ratio in GBM is 5.26, while the average Cho/NAA ratios in normal brain tissue and edema are 0.55 and 0.77, respectively. Therefore, the Cho/NAA ratio of GBM is over 10 times higher than normal brain, which provides a great dynamic range to identify infiltrating tumor cells.

Pre-treatment sMRI identifies high-risk recurrence regions
Abnormalities in brain metabolites, displayed in the ratio map of sMRI, can identify regions at the highest risk for GBM recurrence before beginning radiation therapy. Here, sMRI maps for three patients are shown side-by-side with standard imaging (T1- and T2-weighted MRI). The colored bars indicate the severity of the metabolic abnormalities shown on sMRI. For all patients, the location of abnormalities shown on sMRI was consistent with the first recurrence of GBM. In this way, sMRI may show a “metabolic signature” of tumor that remains after treatment, even when no contrast-enhancing disease appears on standard imaging. Since these “hot spots” can be identified, treating them with targeted radiation therapy based on sMRI, rather than empty resection cavity, could delay recurrence and improve patient outcomes.

Improving chemotherapy for glioblastoma patients
The potent inhibitors of histone deacetylation (HDAC) activity induce redifferentiation of glioblastoma (GBM) shifting its metabolism towards a more normal brain-like state. These drugs also sensitize tumor cells to radiation therapy. For this project, we will establish an important SMRI tool to detect changes in tumor metabolite levels soon after initiation of histone deacetylase inhibitor (HDACi) treatment as a predictor of therapeutic response in GBM patients. Our SMRI-based tool will aid clinicians in identifying early modification of HDACi treatment indicative of favorable response and may allow initiation of alternative therapies at an earlier time if it is clear that HDACi is not effective.
How will sMRI change high dose radiation therapy?
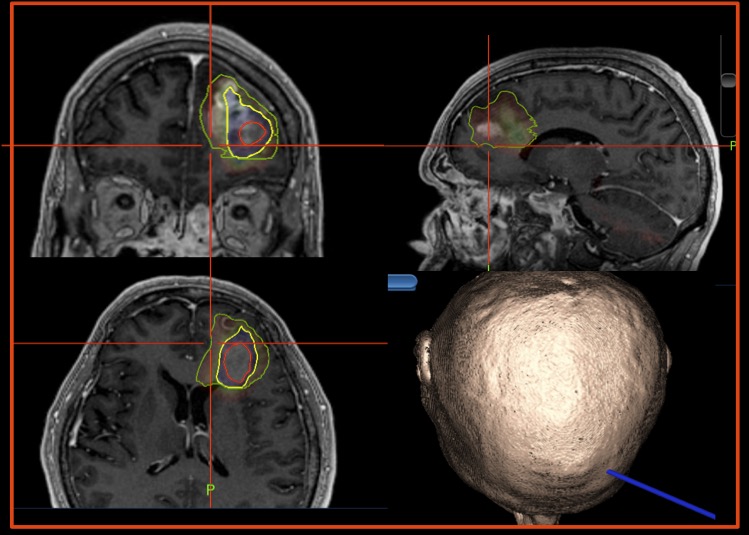
The current standard of care for glioblastoma (GBM) patients is maximal safe resection followed by concurrent radiation therapy and temozolomide chemotherapy. Differences in overall survival depends upon resection status, with the better prognosis occurring when more complete resection of tumor is achieved; otherwise, tumor resection fails to make a meaningful impact on overall survival. Uniquely at our center, we combine Cho/NAA map-based neuronavigation with intraoperative fluorescence-guided surgery to maximize tumor resection.
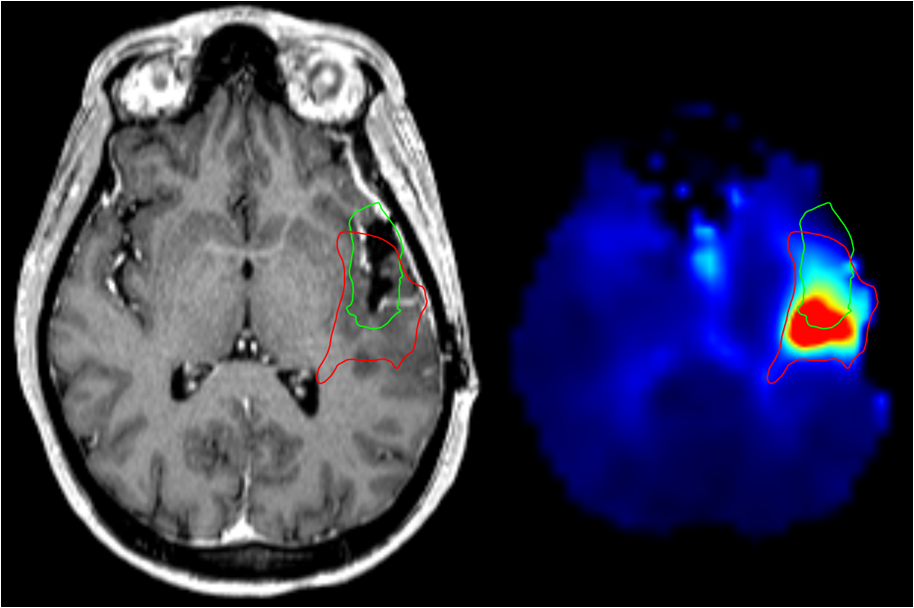
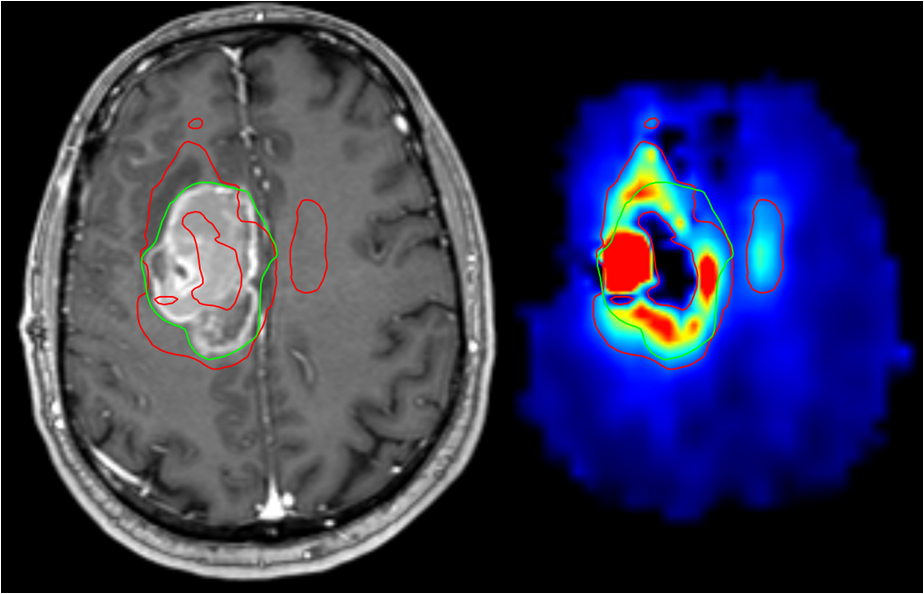
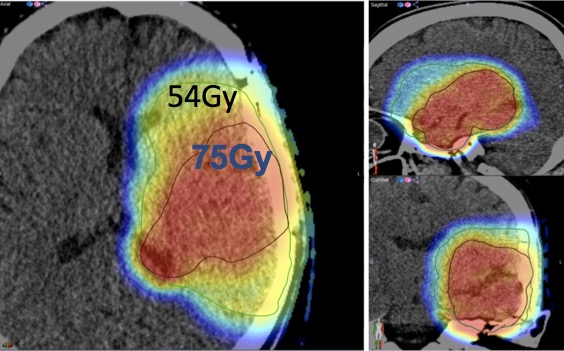
Side-by-side conventional MRI imaging shows radiation therapy boundaries in green, as well as regions of significantly elevated brain metabolite ratios that are associated with tumor spread beyond the standard contrast-enhanced border. The images below highlight the difference in conventional (green) therapy planning and therapy based on metabolic abnormality (red).
Improving radiation therapy targeting for glioblastoma patients
We propose to establish spectroscopic proton magnetic resonance imaging as an important clinical tool to identify regions of brain with significant risk of recurrence of glioblastoma tumor that are not identified by standard MRIs. We believe that our SMRI-based tool will aid clinicians in delineating these regions at high risk for recurrence so that they can be selectively targeted with higher radiation doses than the current standard using regular radiation therapy or Proton beam therapy with the potential benefit of improving outcomes in patients with this highly malignant brain tumor.
Evaluation of high resolution SMRI for biopsy guidance in lower grade gliomas
Diffuse gliomas (astrocytomas and oligodendrogliomas) are devastating tumors that are difficult to manage clinically, in large part due to their widely infiltrative properties and their propensity to undergo malignant progression. Uniquely at Emory, we use volumetric high-resolution whole brain 3D SMRI to predict the most aggressive (anaplastic) regions within these heterogeneous neoplasms, in order to improve the diagnostic accuracy of the stereotactic biopsies, and thus improve the clinical management of these patients.
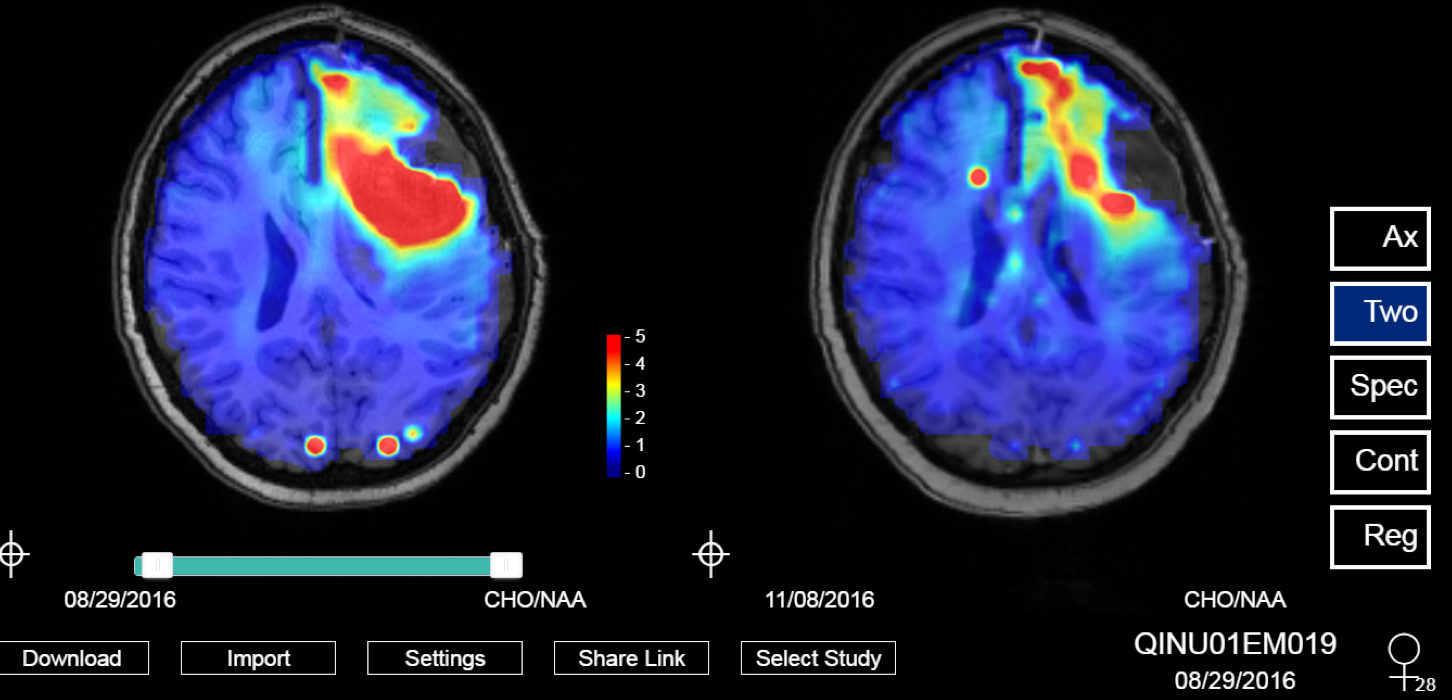
Development of clinically practical SMRI technology
To have our SMRI technology widely available to all the hospitals in the world, we need to come up with an easy (automated) workflow for any MR tech can handle. With the support of the National Cancer Institute [U01 CA172027 (QIN) & F30 CA206291], we are developing an easy-to-use web application for visualization and collaborative treatment planning using spectroscopic MRI. The image below shows a 28 year old female diagnosed with a grade IV brain tumor who was treated with an investigational drug in addition to standard chemo and radiation therapy. The left image is before treatment and the right image is after treatment completion. As the spectroscopic MRI highlights, the metabolic changes show that she positively responded to the therapy (red represents tumor infiltrative activity, blue represents healthy tissue).